
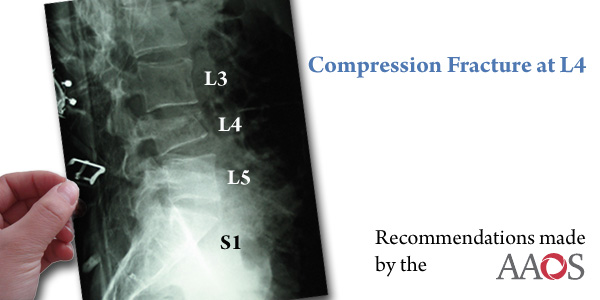
On September 24, 2010, the American Academcy of Orthopaedic Surgery (AAOS) Board of Directors approved new guidelines on the treatment of spinal compression fractures.
Each year over 700,000 people suffer from compression fractures from osteoporosis. Approximately, 1 in 4 people over the age of 50 will suffer from this. Annually, it accounts for 66,000 physician office visits, 70,000 hospitalizations, and over $17 billion spent on treating such fractures in the United States.
Osteoporotic vertebral fractures are defined as any vertebral body height loss of more than 20% from the nonfractured height and by at least 4 mm. These are based on lateral xrays of the spine. Compression fractures can lead to back pain, loss of height, deformity or khyposis, immobilization, and in severe case reduced pulmonary function. These injuries can affect ones activity level, self-esteem, and body image.
Treatment of these fractures is focused on relieving pain, reducing deformity, and improving mobility and function. Surgical and nonsurgical modalities exisit to treat these fractures. Surgical treatment includes minimally invasive procedures such as vertebroplasty (defined as injection of cement directly into the vertebral body) and khyphoplasty (defined as the use of an expandable ballon to reduce the fracture followed by injection of bone filler cement), or in severe case posterior fusion. Nonsurgical treatment consists of braces, pain relievers, bone stimulator (to stimulate bone healing), and exercise. In most cases, these fractures respond well to nonsurgical managment.
The AAOS has made a strong recommendation against vertebroplasty for the treatment of osteoporotic vertebral compression fractures stating, "we recommend against vertebroplasty for patients who present with an osteoporotic spinal compression fracutre on imaging with correlating clinical signs and symptoms and who are neurologially intact." However, the AAOS still considers kyphoplasty to be an option for surgical treatment.
Other recommendations made by the AAOS include (based on weaker research data), use of calcitonin for 4 weeks in patients presenting with acute injury (0-5 days after an identificable even or sudden onset of symptoms); use of ibandronate and strontium relanate as options to prevent additional symptomatic fractures, and the use of L2 nerve root block in spinal compression fractures at L3 or L4 levels.
REFERENCES
(1) Rao RD, Singrakhia MD. Painful osteoporotic vertebral fractures: Pathogenesis, evaluation, and roles of vertebroplasty and kyphoplasty in its management. J Bone Joint Surg Am. 85-A, 2010-2022, 2003.
(2) Lieberman IH, Dudeney S., Reinhardt MD., Bell G. Initial outcome and efficacy of "kyphoplasty" in the treatment of painful osteoporotic vertebral compression fractures. Spine. 26:1631-1638, 2001.
(3) McKiernan F., Faciszewski T., Jensen R. Quality of life following vertebroplasty. J Bone Joint Surg Am. 86-A, 2600-2606, 2004.